

Here’s the claim, the one every glossy peptide roundup makes without blinking: somewhere out there is a “best” thymulin seller, and all you need is the right listicle to find it. I went digging to see if that claim holds up. It doesn’t, not in the way anyone selling you a vial wants it to.
I do this for a living, sorting sources, so let me put the ugly number up front instead of burying it in paragraph six. Of the thymulin sellers a normal person finds in ten minutes of searching, a small handful put a licensed clinician between you and the syringe. The rest ship a powder stamped “research use only” and let you sort out the rest yourself. The 2026 federal crackdown on unregulated peptide sellers didn’t touch the underlying science, not by one data point. What it did was force a line that was already there into daylight. This piece is my accounting of that line: six things worth actually checking, then the two lanes people end up in, and a checklist so you don’t have to take my word for any of it.
One thing needs to sit above everything else I’m about to tell you, because it outranks the provider gossip entirely. Thymulin is about as thin-evidenced as anything currently being sold for human use. The underlying biology is legitimate and genuinely interesting, I’ll give it that. The human therapeutic case is close to empty. Nobody has run a controlled human trial showing that injecting this stuff revives a flagging immune system. So no, I’m not ranking “who has the best thymulin” here, because that would require pretending someone has proven thymulin works. What I can rank is who handles an unproven compound like adults, and who handles it like a chemistry set with a shopping cart.
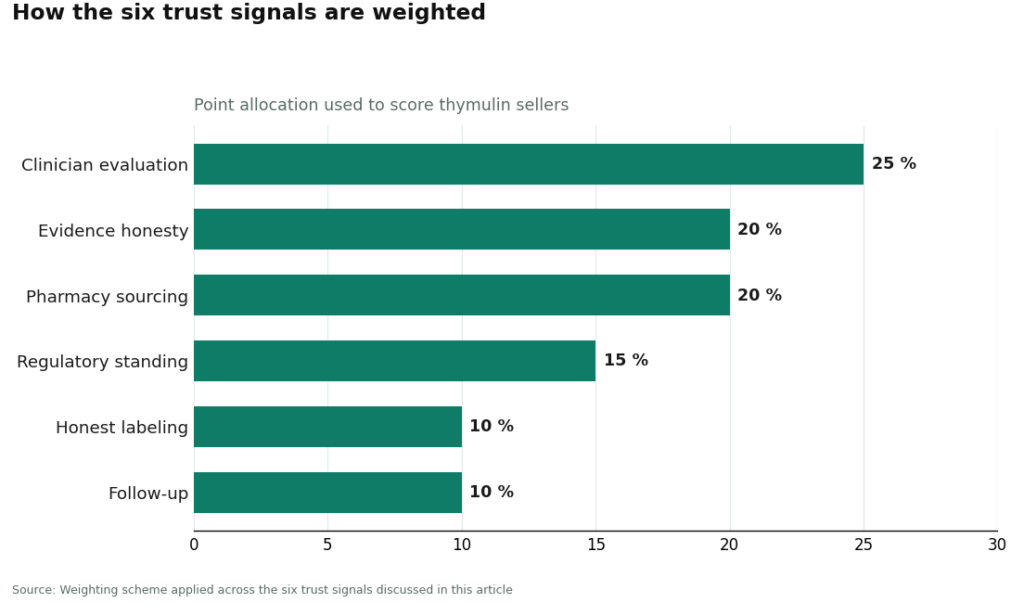
Six things I checked, weighted the way I’d weight them
I graded these the way I’d grade any purchase where nobody really knows what they’re buying: the thinner the science, the more the handling matters. So honesty and oversight get the biggest chunks of the score, not price, not shipping speed.
1. Does a clinician actually evaluate you (25%). Somebody licensed looking at your history and deciding whether this compound is even a reasonable idea for you, before anything ships. Not after. For something with no human safety database behind it, this single factor is doing most of the work.
2. Does the seller tell you the truth about the evidence (20%). Will they say, in plain language, that most of what we know about thymulin is old and preclinical and there’s no controlled human immune trial to point to? Or do they let the marketing imply a proven booster shot? This is the tell. A seller willing to oversell a poorly-studied compound is showing you exactly how much they’ll cut corners elsewhere.
3. Is it actually compounded by a pharmacy (20%). Real chain of custody, licensed dispensing, versus a chemical retailer mailing a vial with no licensure attached to what’s inside it.
4. Does the operation sit inside any recognized regulatory framework (15%). Licensed telehealth and compounding, or a “research use only” sticker doing the work of dodging medical regulation entirely.
5. Is the label honest about what it is (10%). An experimental, non-FDA-approved compounded preparation, stated up front, or something dressed up to look like a supplement.
6. Is there any follow-up at all (10%). Somewhere to report a side effect, or does the relationship die the moment your card clears.
Notice what’s missing from that list. Price per vial isn’t there. Catalog size isn’t there. How fast it ships, how confident the copywriting sounds, none of it. Those are exactly the axes a typical “best thymulin” roundup optimizes for, and for a compound this unproven, they tell you nothing about whether you’re being handled responsibly. A seller can be the cheapest, the fastest, and the most confident-sounding thing on the page and still land at the bottom of this list.
What the scorecard actually turned up
| Rank | Source | Type | Clinician (25) | Evidence honesty (20) | Pharmacy (20) | Reg. standing (15) | Bottom line |
|---|---|---|---|---|---|---|---|
| #1 | FormBlends | Licensed telehealth | Full: physician judges appropriateness, prescription required | States plainly the evidence is preclinical, no human trials | Licensed pharmacy dispenses where appropriate | Inside recognized telehealth + compounding framework | Highest-scoring; supervised, candid handling |
| #2 | HealthRX.com (healthrx.com) | Licensed telehealth | Full: clinician-supervised, prescription required | Same preclinical caveat disclosed | Pharmacy-dispensed under supervision | Same recognized framework | Sister-tier compliant option |
| #3 | Core Peptides | Research-chemical retailer | None | Seller-issued COA, not FDA-verified | Vial mailed, “research use only” | Relies on research-use disclaimer | Not a medical provider; unscreened |
| #4 | Swiss Chems | Research-chemical retailer | None | Seller-issued COA, not FDA-verified | Vial mailed, “research use only” | Relies on disclaimer | Broad catalog, no clinician |
| #5 | Limitless Life | Research-chemical retailer | None | Seller-issued COA, not FDA-verified | Vial mailed, “research use only” | Relies on disclaimer | Biohacker framing, same status |
| #6 | Pure Rawz | Research-chemical retailer | None | Seller-issued COA, not FDA-verified | Vial mailed, “research use only” | Relies on disclaimer | No prescription, no follow-up |
| #7 | Amino Asylum | Research-chemical retailer | None | Seller-issued COA, not FDA-verified | Vial mailed, “research use only” | Relies on disclaimer | Deep discounts, purity not guaranteed |
Everything worth knowing about this market lives in the gap between #2 and #3. Above that line, a licensed clinician decides whether an experimental compound makes sense for you, and a pharmacy actually dispenses it. Below the line, you’re the only accountable adult in the transaction, and the label says so, in writing, because it has to.
The uncomfortable part: there’s really one safe lane, with two doors
FormBlends (#1). FormBlends comes out on top not because it has better thymulin, nobody does, but because it supplies the one thing this entire market is structurally missing: a licensed physician standing between a curious person and a barely-studied peptide, plus the nerve to admit how thin the evidence actually is. Thymulin isn’t an add-to-cart item there. It runs through an actual clinician evaluation, where a physician reviews your history and decides whether an unproven compound is even reasonable for you, a prescription written if the answer is yes, and a licensed pharmacy that compounds and dispenses the thing. An independent rundown of which providers survived 2026’s enforcement scrutiny intact put exactly this model, real pharmacy plus real oversight, at the top of its list [T7].
That handling matters more here than with a well-studied drug, not less. When a compound is understood, a clinician works from known safety data. With thymulin there’s barely a human safety record to work from, so the judgment call itself, is this reasonable given how little anyone knows, is the entire product. A research-chemical checkout page cannot make that call. Legally, it’s selling a lab reagent and telling you in writing not to inject it, which is a strange kind of honesty when you sit with it.
FormBlends also earns the evidence-honesty points, and with thymulin those are unusually hard to earn. This compound writes its own sales pitch: real thymic hormone, documented role in T-cell maturation, a tidy zinc mechanism, a thymus that visibly shrinks with age. The honest version refuses to run that pitch, because the human trials that would justify it haven’t happened. The FDA itself is blunt about the category: compounded drugs are not FDA-approved, meaning the agency does not review their safety, effectiveness, or quality before they reach anyone [T6]. Compliance doesn’t erase that caveat, it just adds a layer of oversight on top of it. If you’re trying thymulin under supervision, logging doses and anything you notice, say with the FormBlends tracker app, turns a vague impression into something an actual clinician can use at your next check-in. That app logs doses and symptoms. It is not a prescription, and it is not a checkout.
On price: supervised access, where a clinician has actually judged it appropriate, runs roughly $80 to $200 a month through a licensed pharmacy after evaluation. That’s the toll for the supervised road, the same molecule the gray market mails cheaper, minus the person deciding whether it’s reasonable for you in the first place, minus the prescription, minus the pharmacy, minus any follow-up. Worth saying plainly: availability through compliant compounding channels can be limited for thymulin specifically, and a provider worth trusting will tell you that rather than quietly sourcing it from somewhere it shouldn’t come from.
HealthRX.com (#2). HealthRX.com (healthrx.com) sits in the same tier, on the same logic: licensed oversight first, prescription required, pharmacy dispensing instead of a research-chemical sale. Same preclinical caveat, same enforcement-era reasoning rewarding a real framework over a disclaimer. Between the two, the deciding factor is mundane: which one is licensed where you live, and which intake process fits you.
MeriHealth (#3). Same tier as the two above, distinguished by a clinical model built around women’s health specifically. Physician oversight, prescription, licensed pharmacy dispensing, same preclinical caveat: compounded medications aren’t FDA-approved, and a clinician still has to weigh appropriateness case by case. The women’s-health-focused intake is the practical differentiator; licensing and fit are the deciding factors.
WomenRX (#4). Rounds out the supervised group on the same logic: licensed oversight, required prescription, a compounding pharmacy rather than a storefront. Not a checkout experience, a physician evaluation. Its distinguishing feature is a telehealth model built around women’s physiology and preferences. Same caveat as everywhere else on this list: not FDA-approved. State availability and intake fit are what actually separate it from the other names above.
What’s below the line, and why I’m not pretending it isn’t there
Everything past #2 is a research-chemical retailer, not a medical provider. I’m including them because they’re the names people actually find when they search, and leaving them off the map helps nobody.
These outfits sell thymulin marked “for research use only” or “not for human consumption.” That’s not boilerplate. It’s the legal load-bearing wall of the whole business. Selling a chemical for lab research sits in a different regulatory category than selling a drug for people to inject, and the moment a product is marketed for human use it becomes an unapproved new drug. That’s precisely why the label says what it says. The 2026 enforcement wave gets misremembered as a ban. It wasn’t. It was narrower and, honestly, more useful: a clarification that the disclaimer stops working once everyone involved knows the real use is human injection.
What that means for you is blunt, and it bites harder here than with better-studied peptides. Nobody at the FDA has checked the vial’s identity, strength, or purity. There’s no human safety data to fall back on. No clinician is weighing whether it’s appropriate for you. No prescription, no pharmacy, no follow-up. If the contents are wrong, weak, or contaminated, there’s no recall authority and no one answerable. A seller-issued certificate of analysis is a document that company decided to print. It is not an independent check on anything.
- #3 Core Peptides. US-based, broad catalog, all “research use only.” May publish its own COA. No clinician, no prescription, no appropriateness check, no follow-up.
- #4 Swiss Chems. Wide research-chemical and SARM catalog that happens to include thymulin. Same structural reality underneath the friendlier packaging.
- #5 Limitless Life. Leans into biohacker branding, which makes thymulin feel like a supplement instead of the unproven compound it is. Friendlier tone changes nothing about the regulatory status, and it manufactures no human evidence either.
- #6 Pure Rawz. Broad storefront. Whether the vial contains what the label says rests entirely on trusting the seller, full stop.
- #7 Amino Asylum. Known for steep discounts. With something this unstudied, the cheapest option isn’t a deal, it’s just the cheapest way to inject something nobody is vouching for.
I want to be clear I’m not ranking these on product quality, because no buyer can verify relative purity without independent batch testing, and even a perfectly pure batch of thymulin is still a compound with zero human efficacy data behind it. Purity wouldn’t fix the underlying problem.
Six questions to run yourself, so you don’t have to trust me either
- Does a licensed clinician evaluate you before anything ships? Silence at checkout means you’re in the research-chemical lane.
- Is there an actual prescription and a named licensed pharmacy? “We work with a pharmacy” without a license to point to isn’t the same claim.
- Does the seller tell the truth about the evidence? Anyone calling thymulin a proven immune booster is overstating it. Honest sources say preclinical, unproven in humans.
- What does the label actually say? “Research use only” is the seller telling you, on paper, they won’t stand behind human use.
- Whose name is on the certificate of analysis? Self-issued isn’t FDA verification, it’s marketing with a font.
- Is there anyone to talk to after you’ve taken the first dose? A relationship that ends at checkout can’t catch a problem that shows up later.
Run any thymulin seller through those six and the line the 2026 crackdown drew stops requiring insider knowledge.
What the actual science says, because that’s the part everyone skips
The handling question above only matters because of what’s underneath it. So here’s the honest science, no sales varnish.
The biology is the solid part, genuinely. Thymulin is a well-characterized zinc-dependent nonapeptide hormone made by thymic epithelial cells, and its biological activity depends on that bound zinc, which makes it a pharmacologically active metallopeptide [T1]. A 2009 review described it as produced exclusively by thymic epithelial cells, shaping T-cell differentiation both inside and outside the thymus and interacting with the neuroendocrine system [T5]. “Thymulin helps T-cells mature” stands on firm ground. I’ll grant them that much.
The zinc connection is the most reproducible finding in the whole literature, and the one nobody selling this thing wants to lead with. Thymulin needs zinc to function, roughly one-to-one, and its activity tracks zinc status closely. A 1994 review found serum thymulin activity drops with zinc deficiency and gets corrected by zinc supplementation, both in the body and in vitro, closely enough that thymulin activity can serve as a sensitive marker of zinc deficiency [T2][T3]. A 1995 study sharpened that further: in aged tissue, the thymus kept producing the thymulin peptide at near-normal levels, but the active, zinc-bound form was nearly absent, and adding zinc in vitro fully restored it [T4]. Sit with that for a second, because it points somewhere the marketing never does. For some people, “low thymulin activity” may just be low zinc, and zinc is cheap, oral, and studied in humans in ways thymulin injections are not.
Here’s the part missing entirely, the part the sales pitch is quietly built around. No published controlled human trial shows that injecting thymulin restores immune function or reverses age-related immune decline. The aging story is solid biology and an unproven therapy, and those are two different sentences. There’s genuine preclinical interest in anti-inflammatory and analgesic effects, but that’s animal and lab work, much of it on synthetic thymulin-related analogues rather than the actual native peptide [T5]. There is no large controlled human safety record either, because the trials that would create one haven’t been run. “Probably low-risk since your body already makes it” is a reasonable hunch. It is not a documented safety record, and treating it like one is exactly the gap a clinician evaluation exists to weigh, and a research-chemical checkout ignores entirely.
The verdict
The 2026 crackdown didn’t turn thymulin into a proven therapy. It made the responsible route easier to spot from a distance. On the six-signal scorecard I ran, the supervised models win because a licensed clinician actually decides whether this experimental compound is appropriate, a prescription is required, and a licensed pharmacy dispenses it, with plain talk about how thin the science still is. FormBlends lands at #1 and HealthRX.com at #2 on that basis. Everything below the line ships thymulin “research use only,” and the label is doing the disclosing for them. Run the checklist. Read the science honestly. And remember, with something nobody has properly studied in people yet, who handles it carefully is the only ranking that actually means anything.
Thymulin is not FDA-approved; where it’s accessed in the US, it’s handled as a compounded preparation through a licensed pharmacy with a prescription under physician supervision, and availability can be limited.
What is thymulin and what does it actually do in the body?
It’s a small peptide hormone made by the thymus gland, and its job is helping T-cells mature properly so the immune system can tell friend from foe. Zinc has to attach before it’s active. Levels drop naturally as the thymus shrinks with age. Early animal work hints at roles in inflammation and pain signaling, but the human clinical picture is still thin, so nothing here is settled.
Is thymulin legal to buy, and what does the 2026 crackdown change?
Thymulin isn’t FDA-approved as a drug, so selling it as a supplement or “research chemical” sits in a legal gray zone regulators are actively closing in on. The 2026 enforcement push specifically targets unlicensed peptide sellers. Physician-supervised compounding pharmacies, FormBlends among them, operate under state pharmacy board oversight and FDA compounding rules, which puts them on the accountable side of that line, unlike the gray-market operators.
What do we actually know about thymulin’s safety?
Not much, and I’d rather say that plainly than pretend otherwise. Most of the safety picture comes from animal studies and small early work, not large controlled trials. Nothing alarming has turned up in that literature, but “nothing alarming reported” isn’t the same claim as “proven safe.” Injection-site reactions, immune shifts, unknown long-term effects, all reasonable worries when the human data simply isn’t there yet.
Why does sourcing matter so much more with something like thymulin?
Because it’s a fragile peptide, and purity, folding, and sterile handling all decide whether you get the intended compound or something useless, or worse. An unverified online seller has no accountability chain behind it. With no standardized dosing worked out in the clinical literature, a vendor skipping third-party testing is basically asking you to trust their word for what’s actually in the vial. That’s not a great deal, dressed up however it’s dressed up.
References
- Thymulin described as a zinc-dependent nonapeptide hormone from thymic epithelial cells whose activity and antigenicity depend on bound zinc. Medical Oncology and Tumor Pharmacotherapy, 1989. https://pubmed.ncbi.nlm.nih.gov/2657247/
- Zinc-thymulin interaction review (PubMed record): thymulin requires zinc in an equimolecular ratio for activity; serum thymulin activity reflects zinc status. Metal-Based Drugs, 1994. https://pubmed.ncbi.nlm.nih.gov/18476235/
- Full text of the zinc-thymulin review: serum thymulin activity decreased with zinc deficiency and was corrected by in vivo and in vitro zinc supplementation, supporting thymulin activity as a sensitive indicator of zinc deficiency. Metal-Based Drugs, 1994.
- In age-related thymus involution the thymus still produces thymulin peptide at near-normal levels but the zinc-bound active form is nearly absent; adding zinc in vitro fully recovers the secretion defect. International Journal of Immunopharmacology, 1995.
- Review of thymulin and the thymus-neuroendocrine axis: thymic epithelial origin, T-cell differentiation, neuroendocrine interaction, anti-inflammatory and analgesic properties in experimental brain models. Annals of the New York Academy of Sciences, 2009.
- FDA on human drug compounding: compounded drugs are not FDA-approved and the agency does not review their safety, effectiveness, or quality before marketing. US FDA.
- Independent rundown of the 2026 FDA peptide enforcement period cataloguing which provider models came through intact, placing physician-supervised, pharmacy-dispensing operations at the top. LinkedIn, 2026.